
Home Pulse Oximetry Could Be Game Changer, Says ER Doc
6 min readWhat your doctor is reading through on Medscape.com:
APRIL 24, 2020 — Clinicians have been combating COVID-19 completely wrong, suggests an unexpected emergency medicine doctor who has been on the front line of the COVID-19 surge in New York Town. “Everybody’s coming in far too late.”
Richard Levitan, MD, invested 10 times in early April working at Manhattan’s Bellevue Medical center Heart at the peak of the COVID-19 surge.
“The x-rays I noticed were all the very same: multi-lobar pneumonia,” he said. “If we could detect it before, we could initiate therapy before. We need to have to improve messaging to the public, to physicians, to get before recognition of the illness.”
Levitan suggests that use of property finger pulse oximeters by individuals with COVID-19 could preempt the precipitous oxygen desaturation that qualified prospects to a crisis that desires intense treatment.
This would considerably lower the recent pressure on hospitals, he told Medscape Professional medical Information.
Levitan argued in a recent New York Periods opinion piece that absolutely everyone desires a pulse oximeter in their pandemic offer kit. The notion strike a nerve: extra than 1500 comments flowed in to the NYT web site, and Levitan’s Twitter feed exploded.
“I believe before detection and therapy will make a big variance,” he said.
But could this kind of a basic, cost-effective system as a finger pulse oximeter be the best weapon in this pandemic? Some industry experts are not certain.
Levitan’s report “is undoubtedly a intriguing theory, but I am not sure that pulse oximetry will be the key to lowering COVID mortality,” David Hill, MD, a pulmonary and crucial treatment professional in Waterbury, Connecticut, and a spokesperson for the American Lung Affiliation (ALA), told Medscape Professional medical Information.
“Levitan’s supposition that individuals who are hypoxemic are respiration extra deeply and creating their have lung injury is a leap,” he said in an email. “Ventilators can lead to lung injury by delivering bigger pressures to the lung, but I am not aware of any facts suggesting amplified respiration in non-intubated individuals with hypoxemia triggers lung injury.”
Crimson Zone vs Blue Zone
Levitan, who is president of Airway Cam Systems, a organization that teaches classes in intubation and airway management in Littleton, New Hampshire, has invested twenty five many years in the field. He has created a graphic illustrating how pulse oximetry could shift the struggle traces to assault an before form of the illness with treatment plans like superior-move nasal cannula oxygen supplementation, constant good airway force (CPAP) equipment, and affected individual positioning/proning.
Continued
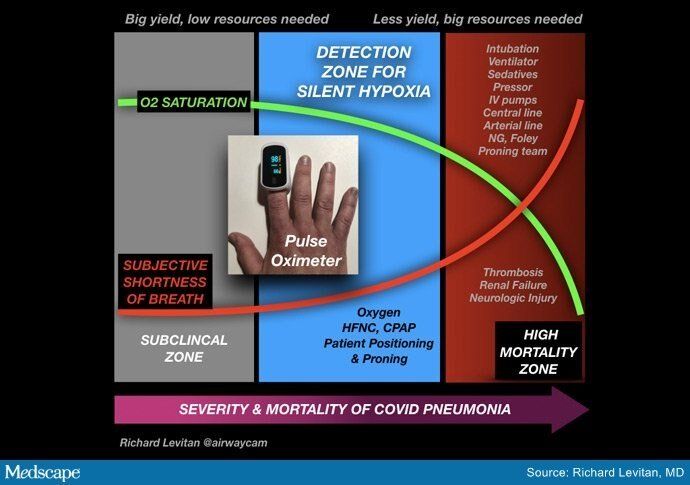
“If we transfer the full window of therapy from the red zone into the blue zone, there will be a logarithmic collapse of the methods wanted to battle this illness. There is no gain combating in the red zone, you can not ramp it up enough. The mortality in the red zone is 70%.
“Clinicians need to have some way to gain,” he additional in an job interview. “Ready for persons to have pulse ox saturations in the 50s and 60s is inquiring for a tsunami of the walking dead.”
But “the walking dead” phenomenon is in fact what ER medical practitioners are at this time reporting with quite a few COVID-19 individuals.
“These individuals did not report any sensation of respiration difficulties, even although their chest x-rays confirmed diffuse pneumonia and their oxygen was below typical,” Levitan details out.
“I am observing individuals with oxygen saturations of 50% ― around equal to what you’d see at the top rated of Everest,” he told Medscape Professional medical Information. “It is wonderful ― shockingly wonderful ― that these persons are alive and speaking on their cell phones.”
Other physicians have also mentioned this and have suggested that some cases of COVID-19 pneumonia resemble high-altitude pulmonary edema (HAPE) somewhat than acute respiratory distress syndrome (ARDS), but industry experts in HAPE have pushed back on that recommendation.
Faster Somewhat Than Afterwards Often Greater?
Erik R. Swenson, MD, a pulmonary professional and professor of medicine at the University of Washington, Seattle, thinks working with a pulse oximeter to detect innovative pneumonia before may well be a superior concept. He routinely advises his individuals to test their oximetry anyway and agrees it should be advised for individuals with COVID-19.
“There is certainly something about this infection that has persons dropping their oxygen stages without the usual distress,” Swenson told Medscape Professional medical Information. “It looks to lead to you to drop that sensation, the typical alarms are not going off, you might be not receiving breathless or tachycardic.
“This is most likely a signal the virus is injuring the lung,” he mentioned. “Without having treatment plans, we don’t know whether or not catching this before is going to make any big variance, but I believe standard concepts would say that catching anything at all sooner somewhat than later is usually far better, and we can usually give oxygen.”
Continued
The ALA’s Hill is extra doubtful about its utility. “Pulse oximetry in the outpatient environment may well recognize individuals who are deteriorating sooner,” he commented. “Undoubtedly in individuals with comorbidities this kind of as cardiac or cerebrovascular illness, it may well be useful to have them arrive to health care awareness sooner and obtain supplemental oxygen.”
However, Hill additional, “I would suspect that the the greater part of individuals who deteriorate with COVID-19 are deteriorating thanks to development of their viral illness and systemic inflammatory response somewhat than silent hypoxemia creating them to improve their respiration and induce lung injury.”
Considerably about COVID-19 is nonetheless not known, he said, and “sudden deterioration in individuals could be thanks to immediate cardiac injury, amplified clotting with cardiac, pulmonary, or CNS results somewhat than progressive silent hypoxemia.”
Nevertheless, Hill concedes that “pulse oximeters are fairly economical (if offered),” and supplying them to individuals with suspected COVID-19 for monitoring “would likely have tiny downside.”
He mentioned, although, that detecting moderate hypoxemia and tachycardia in individuals who would normally do great “could add to supplier workload and potentially ER visits.”
Clients would also need to have to be experienced on correct use, ie, “no nail polish or artificial nails, generating sure their fingers are heat when examining oximetry,” he additional.
A different unexpected emergency doctor, Jeremy Samuel Faust, MD, from Brigham and Women’s Medical center in Boston, who describes Levitan as “a great doc and a pal,” suggests he also has some fears about the public’s reaction.
“Though I believe some pulse oximetry for individuals with a regarded analysis of SARS-CoV-2 makes feeling, I don’t support 50 % the region getting these equipment now on a ‘just in case’ basis,” he told Medscape Professional medical Information. “My concern is that persons who don’t have the virus are getting these in droves now. Like so quite a few issues, there will be shortages, and this will impact the persons that actually have reputable use for these equipment.”
Revenue of pulse oximeters spiked incredibly early in the COVID-19 crisis, according to a report in Quartz, with a extra than 500% improve now in mid-January.
In addition, Faust additional that “as with any property health care tools, there’s usually the concern of above-triage. There is in fact this kind of a issue as examining your figures far too normally. Transient and spurious readings can guide to unnecessary anxiety, and this can send out individuals to clinics and unexpected emergency departments unnecessarily.”
‘)
} else
// If we match equally our test Topic Ids and Buisness Ref we want to position the advertisement in the center of website page 1
if($.inArray(window.s_topic, moveAdTopicIds) > -1 && $.inArray(window.s_small business_reference, moveAdBuisRef) > -1)
// The logic below reads depend all nodes in website page 1. Exclude the footer,ol,ul and table things. Use the varible
// moveAdAfter to know which node to position the Ad container just after.
window.placeAd = function(pn)
var nodeTags = [‘p’, ‘h3′,’aside’, ‘ul’],
nodes,
target
nodes = $(‘.report-website page:nth-baby(‘ + pn + ‘)’).come across(nodeTags.be a part of()).not(‘p:empty’).not(‘footer *’).not(‘ol *, ul *, table *’)
//target = nodes.eq(Math.floor(nodes.duration / 2))
target = nodes.eq(moveAdAfter)
$(”).insertAfter(target)
// At present passing in 1 to transfer the Ad in to website page 1
window.placeAd(1)
else
// This is the default area on the bottom of website page 1
$(‘.report-website page:nth-baby(1)’).append(”)
})()
$(function()
// Create a new conatiner exactly where we will make our lazy load Ad call if the get to the footer section of the report
$(‘.main-container-3’).prepend(”)
)
Pagination



